Blog for CCS/Comprehensive Neuromonitoring written by Rebecca Fingles BS, CNIM
At Comprehensive Neuromonitoring Services (CCS), we value continuous learning and clinical excellence. In this post, we take a closer look at the utility of trapezius muscle monitoring during cervical spine surgery, a topic that has prompted ongoing discussion among neuromonitoring professionals.
Traditionally, when procedures involve the C2-C4 levels, a neuromonitoring technologist would include trapezius muscle monitoring in their EMG and TCeMEP tests. These tests are performed to help the oversight interpreting physician evaluate the motor aspects of a nerve pathway- EMG (Electromyography) by way of passive recording of nerve root activity and TCeMEP (Transcranial electric Motor Evoked Potential) by recording the muscle response conveyed by an evoked stimulation of the brain. Contrarily, there is evidence from studying the Spinal Accessory Nerve (SAN) that deems the trapezius muscle a less than optimal avenue to accurately evaluate the motor function of nerve roots C2-C4.
Anatomy Overview

The trapezius is the large, diamond-shaped muscle that is divided into upper, middle and lower regions. It extends from the base of the skull down the neck, laterally across both shoulder blades, and tapers down the mid-back medially. The muscle is responsible for many upper body movements including shrugging shoulders, head movement, and postural stability. Some researchers refer to the upper trapezius as descending, middle as transverse, and lower as ascending regions.
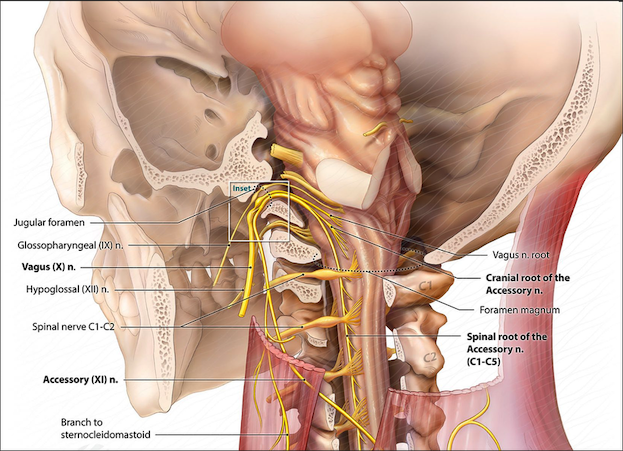
The main motor input for the trapezius muscle comes from the Spinal Accessory Nerve or SAN. Originating in the brainstem as Cranial Nerve XI, the SAN travels through the jugular foramen and descends posterolaterally along the spine to innervate the trapezius and Sternocleidomastoid muscles. The SAN crosses paths with the cervical nerve roots along the way and communicating branches have been identified (2).
Sensory input for the trapezius originates from peripheral nerves that travel to the spinal cord and exit mainly through the ventral rami of C3 and C4.
The Controversy in Monitoring
The controversy in monitoring EMG/MEP for nerve root function during spinal surgery lies in how the motor innervation of C2, C3 and C4 is not always present nor consistent. Multiple studies have demonstrated upon intraoperative stimulation of an intact SAN and using recording electrodes, the upper, middle and lower fibers of the trapezius all contracted in 100% of patients studied (1, 2, 3, 4). By contrast, these same studies showed that stimulation of individual cervical nerve roots C2, C3, C4 only sometimes presented a contraction in the trapezius muscle (1, 2, 3, 4). One of these studies determined that motor input from the cervical plexus to the trapezius muscle was provided in only 32% of cases (2), while another determined motor input to be 39% (3). One study concluded “The SAN provided the most consistent motor input to the trapezius muscle. The C2, C3, and C4 nerves also provided motor input to the trapezius muscle; however, they were either inconsistently present or, when present, irregularly innervated the three parts of the trapezius muscle” (4).
Clinical Implications
The SAN provides the dominant and most consistent motor input to the trapezius muscle, and the SAN is typically not at risk for routine anterior and posterior cervical spine surgeries. Monitoring the trapezius during these surgeries may increase the likelihood of false-positives and may distract from the overall view of patient neuromonitoring. Trapezius muscle monitoring can be most useful during anterior cervical spinal surgeries- placing leads bilaterally in the middle/transverse fibers to detect positional changes in the brachial plexus and upper extremities.
As always, REFER TO YOUR SURGEON when deciding whether to include or omit trapezius EMG/MEP in your neuromonitoring setup – and don’t forget to document!
**Note- I want to mention that I did not have access to full white paper studies when discussing data found in this blog. When studies are mentioned, information is pulled from abstracts and conclusions, along with a comprehensive analysis document for Trapezius utilization in IONM by RTNA referring to some of these studies**
- Pu Y, et al. Trapezius muscle innervation from the spinal accessory nerve and branches of the cervical plexus. Int J Oral Maxillofac Surg. 2008.
- Gavid M, et al. Topographical and functional anatomy of trapezius muscle innervation by spinal accessory nerve and C2 to C4 nerves of cervical plexus. Surg Radio Anat 2016.
- Lind CS, et al. Quantification of trapezius muscle innervation during neck dissections: cervical plexus versus the spinal accessory nerve. An Otol Rhinol Laryngol 2015.
- Kim JH, et al. Motor innervation of the Trapezius muscle: Intraoperative motor conduction study during neck dissection. ORL J Otorhinolaryngol Relat Sepc 2014.